✅Medically reviewed | Updated July 2026
Choosing where to have a P-shot in the UK is not a decision to rush. The market for male sexual health treatments has grown quickly, and quality varies widely between providers. Some clinics offer thorough medical assessment and proper follow-up. Others offer little more than an injection and a receipt. For men researching a Priapus shot London provider, or comparing a P shot treatment against other options for erectile dysfunction, asking the right questions before booking matters as much as the treatment itself.
This article sets out eight practical questions men should ask before choosing a clinic for a P shot. It also explains what the treatment involves, what evidence currently supports it, and where its limitations lie. The aim is balanced, factual guidance, not persuasion.
What Is the P-Shot?
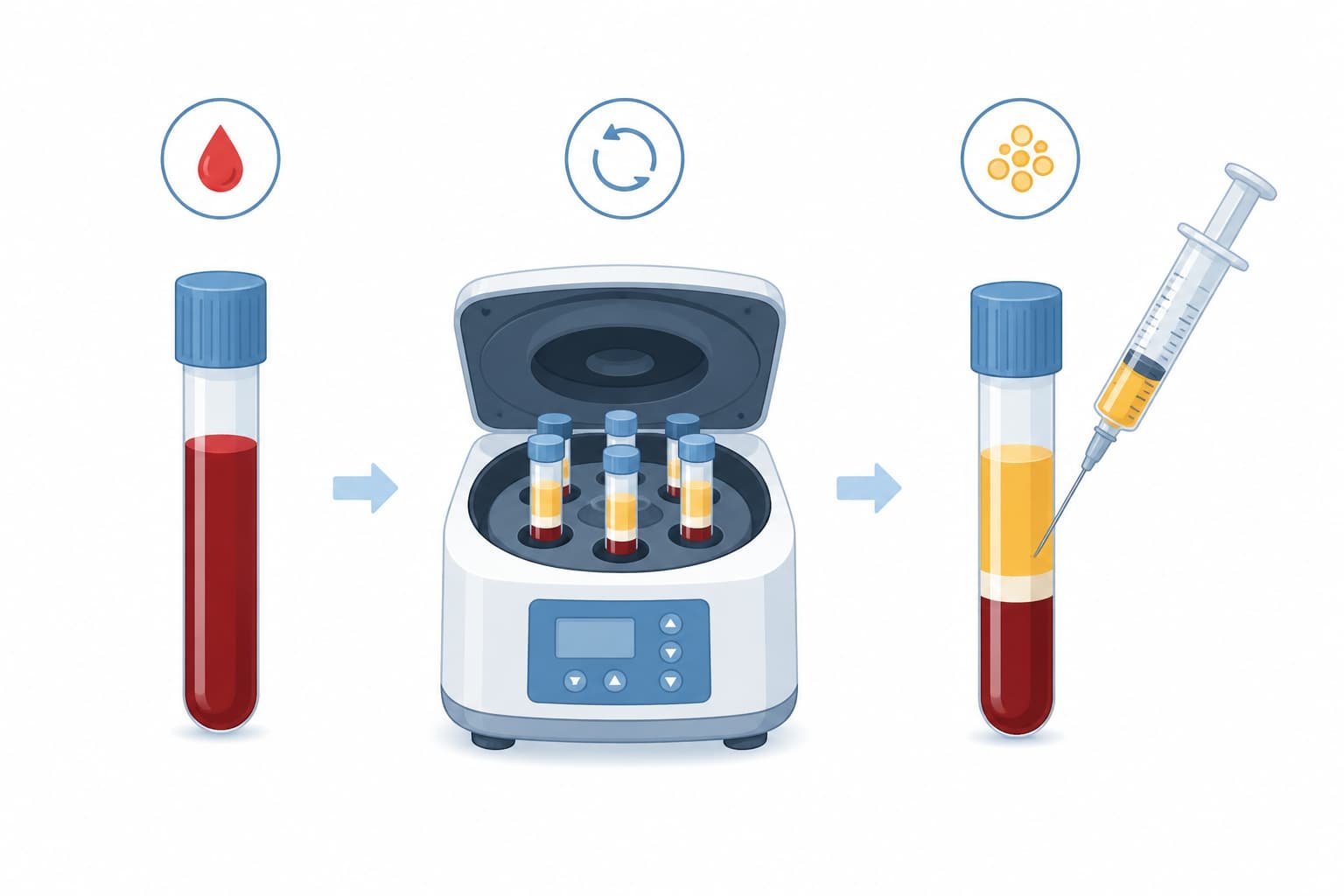
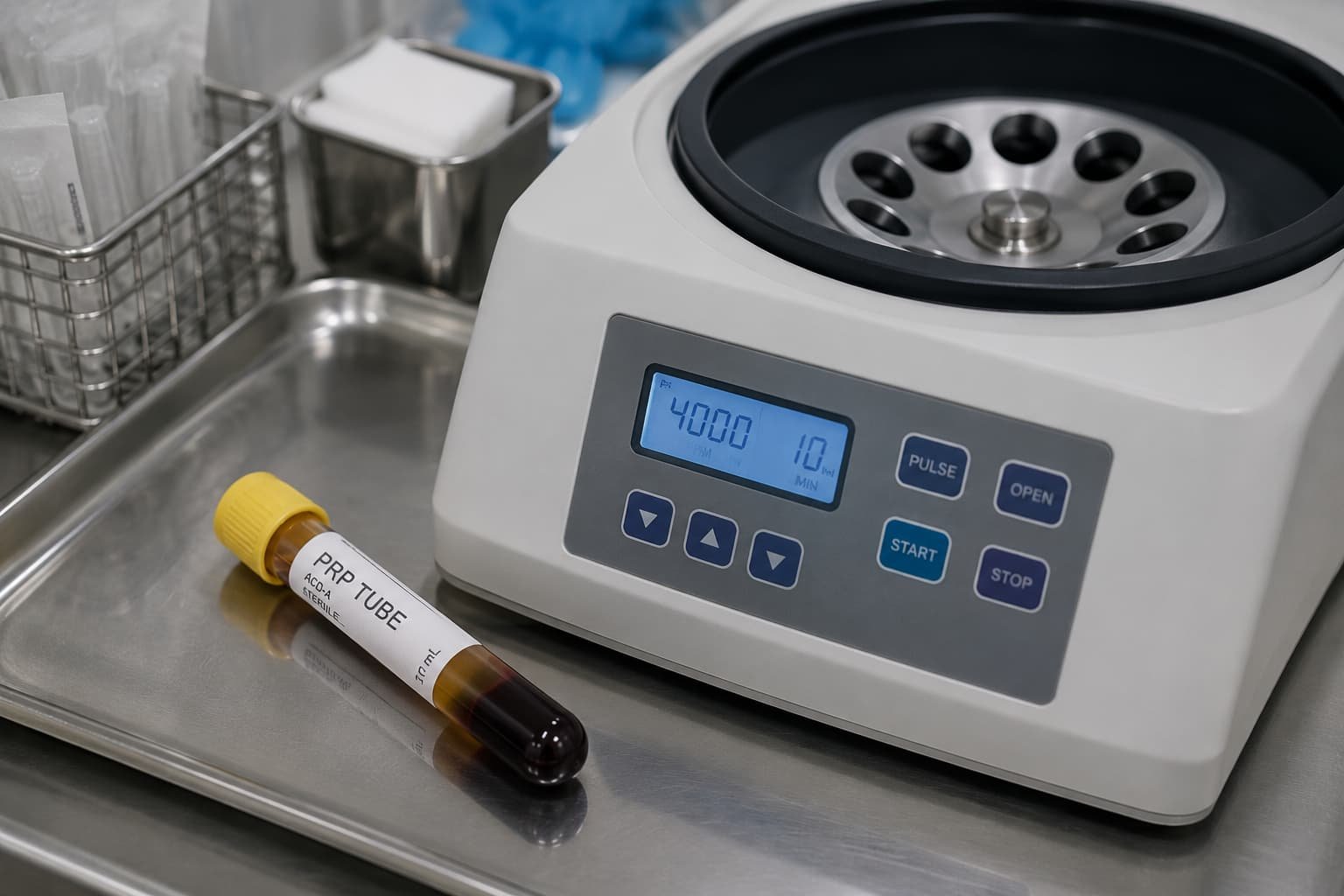
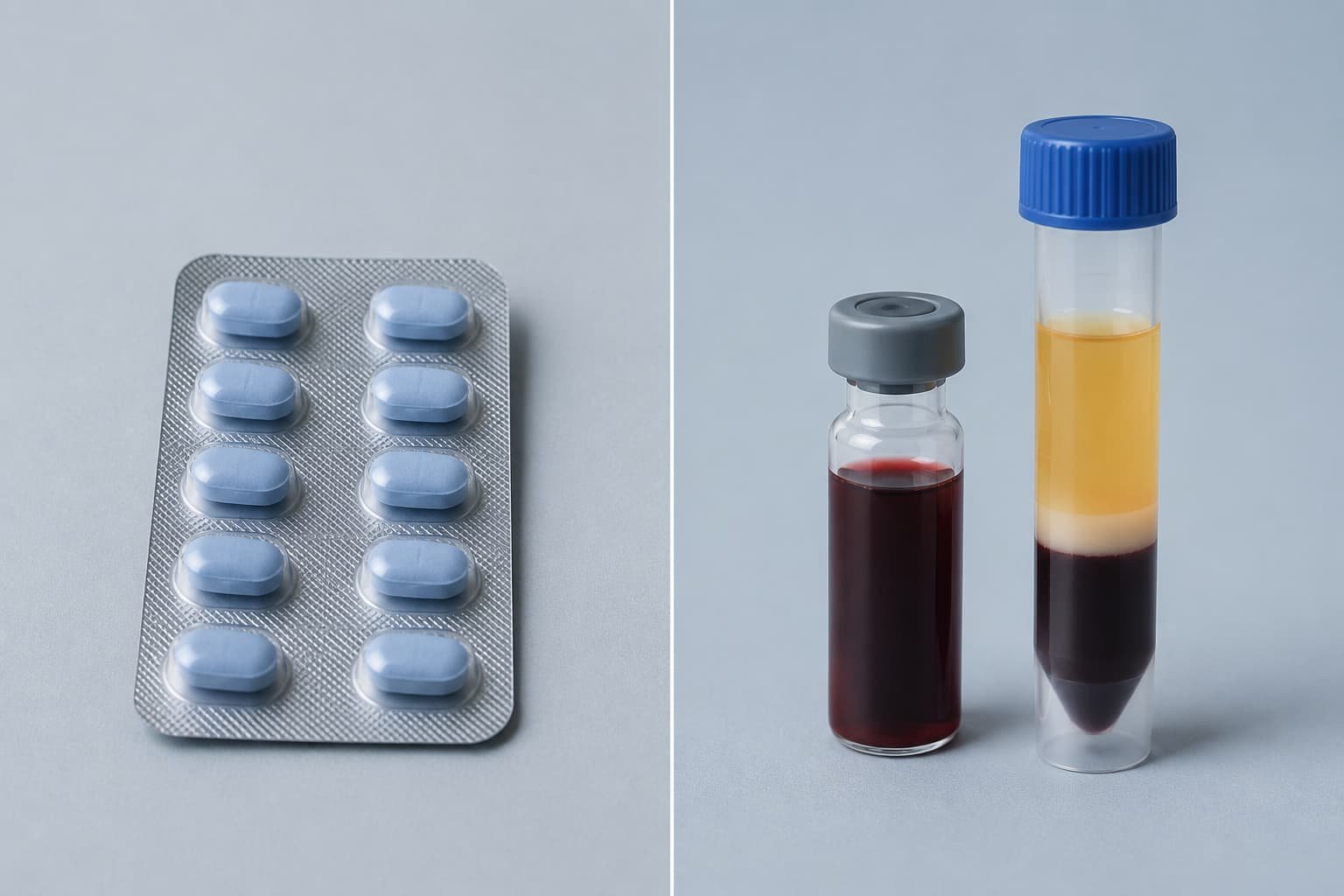
The P-shot, sometimes called the Priapus shot, is a non-surgical treatment for erectile dysfunction in London and elsewhere that uses a patient’s own blood. Clinicians draw a small blood sample, spin it in a centrifuge, and extract the platelet-rich plasma (PRP). This concentrated plasma is then injected into specific areas of the penis.
The theory behind PRP-based regenerative therapy for ED rests on the growth factors contained in platelets. These proteins are thought to stimulate tissue repair and encourage new blood vessel formation. Clinics offering this natural ED treatment using PRP therapy market it as an alternative to tablets, injections of vasodilator drugs, or surgical implants.
It is worth noting that the P-shot is a trademarked term for a specific protocol, though many clinics use PRP-based penile injection growth treatments under similar or generic names. Patients should establish exactly which protocol a clinic follows before proceeding.
Why the Right Clinic Matters More Than the Treatment Itself
The same procedure performed by two different practitioners can produce very different outcomes. PRP preparation techniques vary. Injection technique varies. Aftercare varies. Because the P-shot involves an invasive procedure on sensitive tissue, the skill and training of the practitioner directly affects both safety and results.
The National Institute for Health and Care Excellence (NICE) and the NHS have not issued specific clinical guidance endorsing PRP injections for erectile dysfunction as a standard treatment. This does not mean the treatment lacks value, but it does mean patients cannot rely on an official approval process to vet providers. The responsibility for due diligence sits with the patient.

8 Questions to Ask Before Choosing a P-Shot Clinic
1. Is the Practitioner a Registered Medical Professional?
Confirm that the person performing the injection holds a recognised medical qualification. Ask whether the practitioner is a registered doctor, and check their registration number against the General Medical Council (GMC) register. A P shot UK provider should be transparent about who performs the procedure, not just who owns the clinic.
Non-medical aesthetic practitioners may offer PRP treatments in some settings, but injections involving the penis carry specific anatomical risks. A doctor with relevant surgical or urological training reduces the risk of complications.
2. What Specific Training Has the Practitioner Completed in PRP and Male Sexual Health?
General cosmetic training does not automatically qualify someone to perform genital PRP injections. Ask about specific certification in PRP protocols and in male sexual health procedures. Clinics should be able to describe their practitioner’s training pathway clearly and without evasion.
3. How Is the PRP Prepared, and What Equipment Is Used?
The concentration and quality of platelet-rich plasma depends on the centrifuge system and protocol used. Ask which PRP preparation system the clinic uses and how platelet concentration is measured. Reputable clinics will explain this process in plain terms rather than treating it as a trade secret.
4. What Results Can Realistically Be Expected?
This is the most important question of all. Any clinic that guarantees dramatic or permanent enlargement should raise concern. Evidence for the P-shot remains limited. A small number of peer-reviewed studies suggest modest improvements in erectile function scores and some improvement in penile sensation for certain patients, but sample sizes are small and long-term data is lacking.
Patients researching P-shot before and after results online should treat marketing images with caution. Photographic comparisons are not standardised, and outcomes vary considerably between individuals. A responsible clinic will discuss realistic, modest expectations rather than showing only the most favourable outcomes.
5. What Does the Consultation Process Involve?
A thorough medical history and physical assessment should precede any P shot treatment. This should include screening for underlying causes of erectile dysfunction, such as cardiovascular disease, diabetes, or hormonal imbalance. A clinic that skips this step and moves straight to injection is not practising good medicine.
Erectile dysfunction can be a marker of broader cardiovascular risk. The NHS notes that erection problems sometimes signal underlying heart or blood vessel disease. A responsible provider will not treat symptoms in isolation without considering root causes.
6. What Is Included in the Priapus Shot Price, and Are There Hidden Costs?
Priapus shot price varies across the UK, and cost alone should never be the deciding factor. Ask whether the quoted price includes the consultation, the PRP preparation kit, the injection session, and any follow-up review. Some clinics separate these costs, which can make comparison difficult.
Men comparing male enlargement injections cost UK figures across multiple providers should request an itemised breakdown rather than relying on headline prices. Unusually low prices can sometimes reflect corners cut in preparation quality or practitioner experience.
7. What Aftercare and Follow-Up Is Provided?
Ask what happens after the injection. Is there a follow-up appointment? Is there a clear point of contact if swelling, bruising, or discomfort persists beyond the expected recovery window? Aftercare planning is a strong indicator of a clinic’s overall standard of care.
8. Is the Clinic Registered and Regulated?
Check whether the clinic is registered with the Care Quality Commission (CQC), where applicable, or operates under appropriate medical governance. Ask about the clinic’s complaints procedure and insurance arrangements. Transparency about regulation reflects a clinic’s accountability.
Understanding the Evidence Behind PRP for Erectile Dysfunction

Peer-reviewed research into PRP for erectile dysfunction remains at an early stage. Some small clinical trials report improvements in International Index of Erectile Function (IIEF) scores following PRP injection, particularly in men with mild to moderate erectile dysfunction. Other studies show more limited or inconsistent benefit.
There is currently no large-scale, long-term randomised controlled trial confirming consistent efficacy. NICE has not published a technology appraisal specifically endorsing PRP injection for erectile dysfunction. This does not mean the treatment is ineffective, but it does mean claims should be presented with appropriate caution.
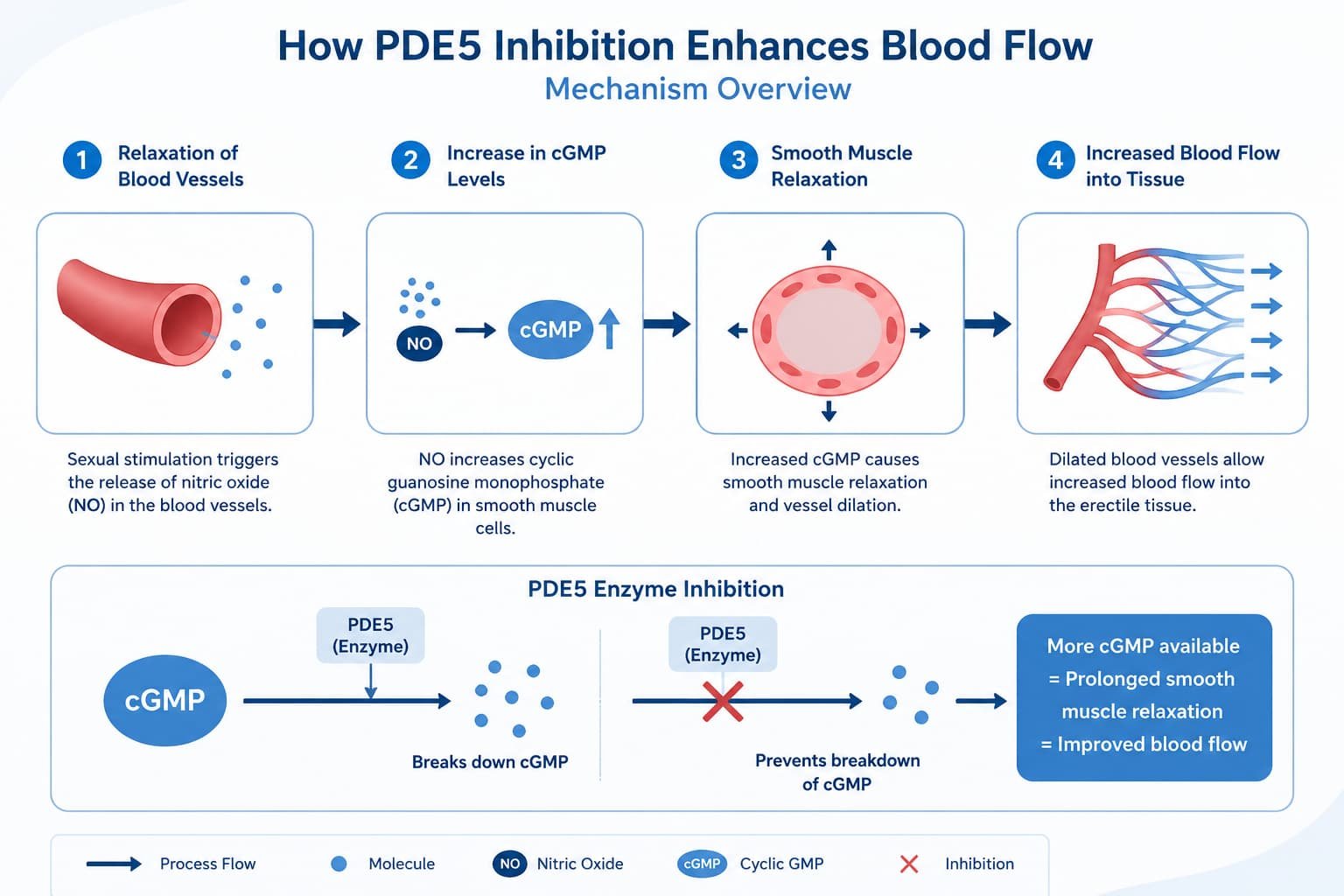
Men considering erectile dysfunction treatment in London clinics offer should discuss all available options with a doctor, including established treatments such as oral PDE5 inhibitors, vacuum erection devices, and, where appropriate, surgical options. PRP therapy may suit some patients as part of a broader treatment plan, but it is not a universal solution.
Who Might Consider This Treatment
The P-shot may be discussed as an option for men experiencing mild erectile difficulty, reduced sensation, or those seeking an alternative to standard pharmacological treatment. It is not typically recommended as a first-line treatment for severe erectile dysfunction, and it is not a treatment for conditions requiring urgent medical investigation.
Men with untreated cardiovascular disease, bleeding disorders, or active infection in the treatment area should not proceed without full medical clearance. A qualified doctor should always make this assessment individually.
Limitations to Understand Before Proceeding
Patients should be aware of several limitations:
- Evidence quality is still developing, with most studies involving small patient groups.
- Results are not guaranteed and vary between individuals.
- Effects, where present, are typically temporary and may require repeat sessions.
- The treatment does not address underlying medical causes of erectile dysfunction, such as vascular disease or diabetes, which require separate management.
A clinic that presents the P-shot as a guaranteed or permanent solution is not providing balanced information.
The Role of Clinical Governance in London’s Private Sector
London, particularly the Harley Street and Marylebone area, hosts a concentration of private clinics offering aesthetic and sexual health treatments. This concentration reflects strong demand but also means standards vary considerably between providers. Pshots Clinic, based in this area under the clinical leadership of Dr Syed Nadeem Abbas, is one example of a provider operating within this private healthcare landscape, illustrating the range of practitioner backgrounds patients may encounter when researching options.
Patients should not assume that a Harley Street address alone signals a particular standard of care. Location is not a substitute for verified qualifications and transparent practice.
Making an Informed Decision
Choosing a provider for a P shot requires the same diligence as choosing a provider for any medical procedure. Verifying qualifications, understanding realistic outcomes, and asking direct questions about preparation and aftercare protects patient safety. A cautious, questioning approach benefits every patient, regardless of which clinic they eventually choose.
Frequently Asked Questions
Is the P-shot approved by the NHS?
The P-shot is not currently offered on the NHS and is available only through private clinics. NHS guidance does not formally endorse PRP injection for erectile dysfunction as standard treatment.
How long do P-shot results last?
Where benefits occur, they are generally reported as temporary. Some patients seek repeat sessions, though clinical data on optimal frequency remains limited.
Is the procedure painful?
Local anaesthetic is typically used to reduce discomfort during injection. Some soreness or bruising afterwards is commonly reported.
Can the P-shot cure erectile dysfunction permanently?
No. Current evidence does not support claims of a permanent cure. It may help manage symptoms in some patients as part of a wider treatment approach.
How much does a P-shot cost in the UK?
Pricing varies by clinic and by what is included in the package. Patients should request a full, itemised cost breakdown before booking.
Conclusion
Selecting a clinic for a P shot should never be based on price or convenience alone. The eight questions outlined above give patients a practical framework for assessing practitioner qualifications, treatment quality, and realistic expectations. Because clinical evidence on PRP for erectile dysfunction remains limited, informed, cautious decision-making protects both safety and outcomes.
Given the current gaps in long-term evidence, how much weight should patients place on individual clinic testimonials when deciding whether this treatment is right for them?
Read more: How to Prepare for a P-Shot: Full Pre-Treatment Checklist