✅Medically reviewed | Updated July 2026
Cycling ranks among the most popular forms of exercise in the United Kingdom. It supports cardiovascular fitness, weight management and mental wellbeing. Yet persistent reports link prolonged bike riding with genital numbness. Some riders also report erectile difficulties. This raises genuine concern about cycling erectile dysfunction among regular riders.
Current medical literature does not confirm that cycling directly causes erectile dysfunction. Certain riding patterns and equipment choices still carry measurable risk. This article examines the neurovascular mechanisms involved. It reviews the strength of existing evidence. It also outlines practical prevention strategies. The article explores an established non-surgical treatment for erectile dysfunction in London, including PRP-based regenerative therapy for ED. Men who continue to experience symptoms may find this useful, regardless of the underlying cause. Men researching treatment options will find both perspectives addressed below.
Understanding the Cycling Erectile Dysfunction Connection
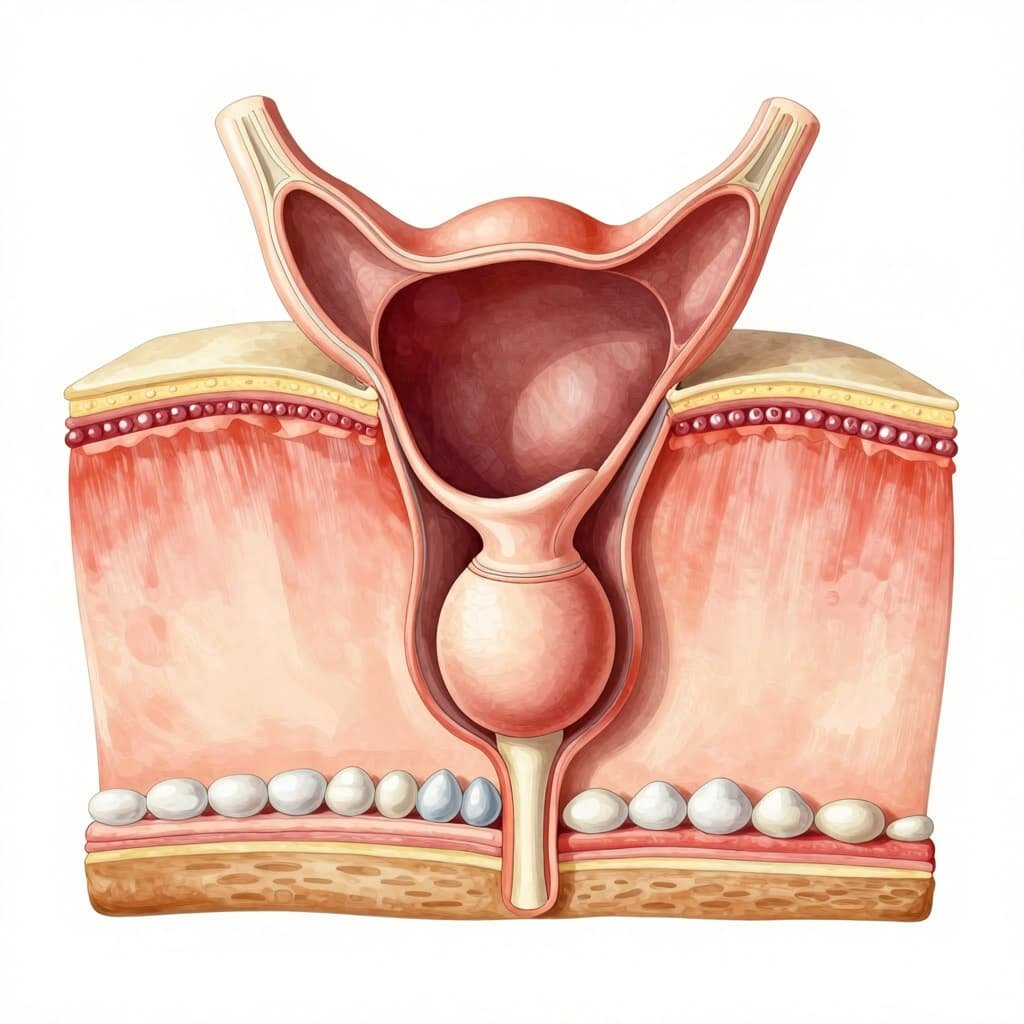
The perineum sits between the base of the penis and the anus. It carries a dense network of blood vessels and nerves. During cycling, body weight rests largely on this narrow region. The sit bones are designed for weight-bearing instead. Traditional saddle shapes concentrate pressure directly onto the perineal area. This compresses structures that supply blood and sensation to the penis.
How Saddle Pressure Affects Blood Flow and Nerves
Sustained compression reduces oxygen delivery to penile tissue during longer rides. Early clinical studies measured penile blood pressure after saddle sitting. Reductions to around 60 per cent of baseline appeared within five minutes.
Blood flow typically returns to normal within ten minutes of recovery. This indicates the effect is usually transient rather than permanent.
The Role of the Pudendal Nerve and Artery
The pudendal nerve and pudendal artery both pass beneath the pubic bone. They travel through a narrow channel known as Alcock’s canal. Prolonged saddle pressure compresses these structures. This produces numbness, tingling or reduced sensitivity. Repeated compression over months or years has been linked to pudendal nerve injury. These links come from isolated case reports. Direct causation across the general cycling population remains unproven.
Types of Cycling and Relative Risk
Not all forms of cycling carry equal risk to penile blood flow and nerve function. Road cycling over long distances generates the highest recorded perineal pressures. Drop handlebars increase forward pelvic tilt and add to this risk. Upright commuter cycling and short recreational rides produce lower pressure. These shorter rides also involve shorter periods of compression.
Indoor Spin Classes and Static Bikes
Indoor spin classes often involve a fixed, forward-leaning position. This position is sustained for 45 minutes or longer. Road surface variation normally offers natural pressure relief outdoors. Static bikes indoors do not provide this relief. Static bike setups in gyms are rarely fitted individually. This can increase saddle pressure when bike geometry does not match a rider’s proportions.
Mountain Biking and Off-Road Cycling
Off-road cycling introduces frequent shifts in body position. Standing climbs and variable terrain interrupt sustained perineal pressure. This intermittent loading pattern may reduce cumulative compression. Continuous road riding does not offer the same relief. Rougher terrain also increases vibration transmitted through the saddle.
Electric Bicycles
Electric bicycles reduce the physical effort required per mile. This can shorten time spent under load for a given journey. Riders using e-bikes for daily commuting accumulate less total saddle time. This lowers overall exposure to perineal compression compared with endurance training.
What the Evidence Actually Shows
Cycling Duration and Cumulative Risk
Elevated cycling erectile dysfunction risk appears concentrated among high-mileage cyclists. Casual or moderate riders show lower risk levels. One frequently cited study reported genital numbness in 61 per cent of male cyclists. The same study found erectile dysfunction in 24 per cent of these men. Their weekly training exceeded 400 kilometres.
Recreational cyclists covering shorter, less frequent distances show substantially lower rates of reported symptoms.
Cycling Versus Other Forms of Exercise
Comparative studies show similar erectile function scores across different exercise groups. Recreational cyclists, swimmers and runners scored closely in these studies. Cyclists did report more genital numbness than other groups. This pattern suggests cycling alone does not universally cause erectile dysfunction. Cumulative saddle pressure, riding position and bicycle fit appear more influential than the activity itself.
Recognising the Warning Signs
Genital Numbness
Numbness lasting only during or shortly after a ride is common. This is generally not a cause for concern.
Numbness persisting beyond 24 hours after dismounting warrants medical assessment. It may indicate more significant nerve compression.
Persistent Erectile Difficulties
Erectile difficulties unrelated to specific rides deserve proper investigation. The same applies to symptoms that worsen despite equipment adjustments. Erectile dysfunction frequently signals underlying cardiovascular disease. Penile and coronary arteries share similar blood vessel pathways. Men presenting with new erectile difficulties should undergo cardiovascular risk assessment. This should sit alongside urological review. NICE guidance recognises erectile dysfunction as a potential early marker of vascular disease.
Reducing the Risk of Cycling Erectile Dysfunction
Saddle Design and Bike Fit

Saddles featuring a central cutout redistribute pressure away from the perineum. This shifts weight toward the sit bones instead. Professional bike fitting adjusts saddle height, tilt and handlebar reach. These adjustments reduce forward pelvic tilt. Forward pelvic tilt is known to increase perineal loading.
Standing and Positional Changes

Standing on the pedals every ten minutes restores blood flow to compressed tissue. This applies especially during longer rides. This simple habit is supported by available evidence. It offers a low-cost, practical prevention strategy for regular cyclists.
Riding Frequency and Recovery
Rest days between long rides allow perineal tissue to recover fully. Gradual increases in distance reduce cumulative strain on nerves and blood vessels. Sudden jumps in weekly mileage do not allow the same recovery. Padded cycling shorts distribute pressure across a wider surface area. They also reduce friction during longer rides. Padding alone does not replace correct saddle selection. Bike fit remains the primary preventive measure.
When Cycling Habits Are Not the Only Factor
Erectile dysfunction rarely stems from a single cause. Cardiovascular disease, type 2 diabetes, smoking and obesity all raise risk. Psychological stress remains a factor too. These causes are typically stronger than cycling for most men.
NICE guidance recognises erectile dysfunction as an early marker of cardiovascular disease, particularly in men under 60. Addressing modifiable risk factors forms the foundation of NHS management pathways. These factors include blood pressure, cholesterol and blood glucose control. This groundwork comes before any procedural intervention is considered.
Standard NHS Assessment Steps
A GP consultation for erectile dysfunction typically includes blood pressure measurement. Blood tests for glucose and cholesterol usually follow. A review of current medication also forms part of this process. Testosterone levels may be checked where low libido accompanies erectile symptoms. These steps identify or exclude systemic causes. This happens before cycling habits are considered a primary factor.
First-Line NHS Treatment Options
First-line management usually involves oral phosphodiesterase type 5 inhibitors. Lifestyle modification supports this approach. This includes reduced alcohol intake, smoking cessation and increased activity. Cycling itself remains part of a cardiovascular-protective exercise routine. It is not typically discouraged outright, even when saddle-related symptoms are present.
Non-Surgical Treatment for Erectile Dysfunction in London

Men experiencing persistent erectile difficulties may explore other options. This applies whether symptoms link to cycling, vascular disease or age-related decline. Regenerative treatment for male health in the UK offers an alternative approach. It differs from oral medication or surgical intervention. PRP therapy for men’s performance issues has attracted growing clinical interest. It works through tissue repair mechanisms rather than temporary symptom masking. This positions it as a non-surgical treatment for erectile dysfunction in London.
PRP-Based Regenerative Therapy for ED

PRP-based regenerative therapy for ED uses a concentrated fraction of blood platelets. These platelets come from the patient’s own blood. They are rich in growth factors that support tissue repair. This natural ED treatment using PRP therapy aims to stimulate new blood vessel formation. It also supports nerve tissue within penile tissue.
Platelets contain growth factors including platelet-derived growth factor and vascular endothelial growth factor. Both factors play a role in tissue healing across regenerative medicine. Applying this platelet fraction into penile tissue theoretically supports repair of affected neurovascular structures. These are the same structures affected by prolonged saddle compression. Robust, large-scale clinical trial data specific to erectile dysfunction remains limited.
The approach forms the basis of men’s intimate health treatment in London. It sits under the trademarked name Priapus Shot, commonly known as the P shot or Pshot. Men researching this option frequently search for P shot London providers. These providers offer the regenerative technique alongside standard erectile dysfunction treatment London pathways.
The P Shot Procedure Explained
The P shot treatment is also referred to as the P injection. It involves injecting processed platelet-rich plasma into specific areas of the penis. A P shot London clinic typically extracts blood first. The clinic then processes it to isolate platelets. The P injection is administered under local anaesthetic. The priapus shot procedure usually takes under an hour. It requires minimal downtime.
P shot London providers position this penis shot as a regenerative option. This applies to men seeking improved erectile firmness and sensitivity. It is not a guaranteed cure for underlying vascular or nerve damage. Suitability depends on individual clinical assessment.
P Shot Before and After: Realistic Expectations
P shot before and after outcomes vary between patients. Results depend heavily on the underlying cause of erectile difficulty. P-shot before and after results are not immediate. Visible changes typically develop over several weeks as tissue repair progresses.
Penile injection growth claims associated with the P shot remain limited by available clinical evidence. Results should not be equated with surgical enlargement techniques. Men considering P shot UK treatment should discuss realistic expectations first. This discussion should happen with a qualified practitioner before proceeding. Men should also review documented P shot London before and after cases. This forms part of an informed decision.
Priapus Shot Price and Considerations in the UK
Priapus shot price varies across P shot London clinics. Practitioner experience, technique and aftercare provision all affect cost.
Male enlargement injections cost UK figures should always be weighed against practitioner qualifications. Price alone should not guide this decision. A reputable Priapus shot London clinic provides thorough consultation. The clinic confirms suitability and outlines evidence limitations before treatment begins.
Pshots clinic in UK , is led by Dr Syed Nadeem Abbas. The clinic offers P shot treatment alongside broader erectile dysfunction assessment. This includes cardiovascular and lifestyle review where clinically appropriate.
Frequently Asked Questions
Is cycling erectile dysfunction a confirmed medical diagnosis?
This is not a formally confirmed, universal diagnosis. Risk appears linked to prolonged duration, high saddle pressure and poor bike fit.
How long should genital numbness last after cycling?
Numbness should resolve within minutes to hours after a ride ends. Numbness persisting beyond 24 hours requires medical review.
Can changing the saddle prevent erectile problems?
Saddles with a central cutout reduce perineal pressure in several studies. They also lower symptom rates for many riders. Saddle change alone does not guarantee complete symptom resolution for every rider.
Is a P shot suitable for cycling erectile dysfunction?
Suitability depends on the underlying cause and severity of symptoms. A P shot London consultation determines whether PRP-based regenerative therapy for ED is appropriate.
When should a GP be consulted about erectile dysfunction?
New, persistent or worsening erectile difficulties warrant GP assessment. This matters particularly given the established links to cardiovascular disease.
Does stopping cycling reverse erectile dysfunction?
Symptoms caused by temporary compression typically improve once saddle pressure is removed. Adjusting riding habits also supports recovery. Erectile dysfunction with a vascular or systemic cause requires separate medical management. This applies regardless of cycling habits.
What is the difference between the P shot and standard ED medication?
Oral medication temporarily improves blood flow for a single sexual event. The P shot uses PRP to target tissue repair over time. It works through a different mechanism with a separate evidence base.
Key takeaways
Cycling offers substantial cardiovascular and metabolic benefits for most riders. These benefits generally outweigh the sexual health risks involved.
Current evidence indicates cycling erectile dysfunction is usually temporary rather than permanent. This applies provided saddle pressure and riding duration remain within reasonable limits. Persistent symptoms deserve proper medical investigation rather than assumption or self-diagnosis.
Men experiencing ongoing erectile difficulties benefit from informed discussion of all available options. This applies whether difficulties stem from cycling, vascular disease or other causes. Options include P shot London treatment as one non-surgical treatment for erectile dysfunction in London. Several evidence-based pathways exist alongside this option.
What steps might reduce cumulative saddle pressure without losing cycling’s health benefits?
Read more: How Lifestyle Affects P Shot UK Results – Diet, Exercise, and Sleep
Platelet-Derived Growth Factor in PRP: How It Helps Repair Penile Tissue